



 |
市場調查報告書
商品編碼
1114725
ER+/HER2-轉移性乳癌(mBC)市場:1次調查(KOL的洞察) - 市場情報 - 流行病學和到2032年的市場預測ER+/HER2- Metastatic Breast Cancer (mBC)| Primary Research (KOL's Insight) | Market Intelligence | Epidemiology & Market Forecast-2032 |
||||||
全球ER+/HER2-轉移性乳癌(mBC)的市場規模,預計2018年~2032年的調查期間中以6.6%的年複合成長率擴大,至2032年成為158億美元。
本報告提供全球ER+/HER2-轉移性乳癌(mBC)市場相關調查,市場現狀,以及病例數趨勢,患者趨勢,競爭產品的市場上地位,市場機會等資訊。
目錄
摘要整理
ER+/HER2-轉移性乳癌(mBC)疾病的背景
- ER+/HER2-轉移性乳癌定義
- 症狀和原因
- 病因
- 分期
ER+/HER2-轉移性乳癌(mBC)的診斷
流行病學和患者族群
ER+/HER2-轉移性乳癌(mBC)的流行病學和模式參數的主要資訊來源
- 美國
- 德國
- 法國
- 義大利
- 西班牙
- 英國
- 日本
目前治療方法和醫療行為
ER+/HER2-轉移性乳癌(mBC)-治療研究
未滿足需求
ER+/HER2-轉移性乳癌(mBC)-成藥
新的治療方法
ER+/HER2-轉移性乳癌(mBC)-價格與償付
未來的治療範例
現在及新治療方法的年度費用
市場預測
到2032年的各國市場預測
- 主要醫藥品市場上ER+/HER2-轉移性乳癌(mBC)的治療藥銷售額,2018年~2032年
- ER+/HER2-轉移性乳癌(mBC)治療的各患者佔有率和藥物
各國市場預測
- 美國
- 德國
- 法國
- 義大利
- 西班牙
- 英國
- 日本
市場促進因素與阻礙因素
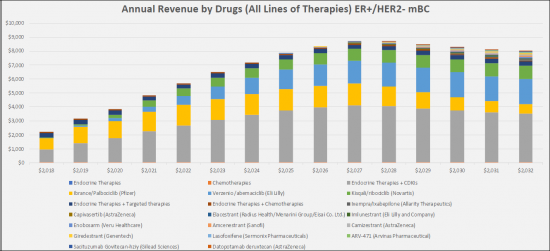
The ER + / HER2- metastatic breast cancer (mBC) market is relatively large with the highest market share holding CDK4 / 6 drugs, e.g. Pfizer's Ibrance (palbociclib), Novartis's Kisqali (ribociclib) and Eli Lilly's Verzenio (abemaciclib). By 2032, these drugs will continue to hold the largest share of the market, but we also expect the market to expand with the addition of new oral SERDs/SARMs/SERMs that will take a combined share of 19.1%, antibody drug conjugates with a share of the 2.9% and AKT inhibitors with a 2.6% share. The sales of the emerging therapies for the treatment of ER+/HER2- mBC in the study countries (United States, France, Germany, Italy, Spain, United Kingdom and Japan) will experience high growth over the 2022-2032 study period, adding a value estimated at a total market of $ 5.6 billion by 2032.
"Currently, -50% of ER+/HER2- mBC patients that are treated with ETs develop resistance or don't respond to initial ET. Endocrine therapies (Els) have advanced the care of patients with ER+/HER2- mBC, yet due to complex tumor mechanisms and endocrine resistance, progression still persists."
Breast cancer tumors are considered estrogen receptor (ER) and/or progesterone receptor (PR) positive if ≥1% of tumor cell nuclei are immunoreactive. Breast cancer cells that have receptors for either hormone are considered hormone receptor-positive (HR+), or just hormone-positive. Breast tumors may be positive for estrogen receptors (ER+), progesterone receptors (PR+) or both (ER/PR+). About 80 percent of all HR+ breast cancers are ER+ or ER/PR+. The average age at diagnosis for people with Breast cancer is 64, and most people are diagnosed between the ages of 62 and younger. ER+ breast cancer is not common in people younger than age 45.
Generally, the type of breast cancer a woman has governs her treatment choices. Tumors that express estrogen receptors (ER+) grow in the presence of estrogen. They are usually treated with endocrine therapy that blocks estrogen from attaching to estrogen receptors, thereby slowing tumor growth. Once the cancer has progressed to the metastatic setting, treatment is generally not curative and the goal is to prolong patients' lives, delay disease progression and minimize cancer-related symptoms.
Currently, overcoming acquired endocrine therapy resistance and improving efficacy outcomes in the 2L+ setting remains a key unmet need in the treatment of ER+/HER2- Metastatic Breast Cancer. A number of SERDs in development have shown improved anti-tumor activity compared to fulvestrant in tumors with ESR1 hotspot mutations that are resistant to AIs. Emerging Protein degraders may be well positioned to overcome resistance as they degrade the estrogen receptor rather than inhibit its action, and they only need to maintain transient binding
ER+/HER2- Metastatic Breast Cancer (mBC)- Epidemiology
The total incidence cases in the G7 countries are anticipated to rise to 290,458 cases by 2032 for the study period (2018-2032). As per estimates, the the United States accounted for the highest incident of ER+/HER2- Metastatic Breast Cancer (mBC) cases in 2018 which was 49,239 cases and are expected to reach 53,540 cases by 2032 with a CAGR of 0.6% for the study period. Among the EU5, Germany had the highest ER+/HER2- Metastatic Breast Cancer (mBC) cases, followed by the France, UK, Italy and Spain. Japan is reported to have the highest number of cases after United States. Japan is reported to have the highest number of cases after the United States.
At the time of diagnosis, approximately 90% of breast cancers are not metastatic; however, in addition to the 10% metastatic at diagnosis, approximately 10-60% of localized breast cancers develop systemic relapse. Furthermore, the prognosis for ER+ mBC is a median five-year survival rate of 27%.
The 5-year relative survival rate is approximately 98.4% for women with localized breast cancer, although the rates decrease to approximately 90.7% for patients with regional involvement and 39.3% for patients with distant metastasis. Breast cancer management depends on biomarkers including estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 (ER/PR/HER2). ER is an important prognostic biomarker in breast cancer. ER-positive tumors have a better prognosis than ER-negative tumours. Overall survival, disease free survival, recurrence/relapse-free survival, 5-year survival, time to treatment failure and time to recurrence have all been shown to be positively associated with ER expression.
ER+/HER2- Metastatic Breast Cancer (mBC)- Current Market Size & Forecast Trends
The estrogen receptor-positive and human epidermal growth factor receptor 2 negative (ER+/HER2-)metastatic breast cancer (mBC) therapeutics market is expected to experience high growth throughout our study period (i.e. 2018 to 2032) to USD 15.8 billion, representing compound annual growth (CAGR) of 6.6%.
The current therapies market to treat ER+/HER2- metastatic Breast Cancer (mBC) is large in the G7 Countries (United States, European 5 countries and Japan). The United States captured the highest market share in 2022 as compared to European 5 countries and Japan. We expect that with the launch of the new therapies, the current treatment landscape will grow, catering to the need of the metastatic patient's group in all lines.
Endocrine therapy (ET) remains the backbone of treatment in these cases, improving survival and quality of life. However, treatment can lose effectiveness due to primary or acquired endocrine resistance. The ER+/HER2- cases are typically treated with endocrine therapy (ET), such as selective estrogen receptor inhibitors and aromatase inhibitors (AIs). Although ET remains the backbone of HR+ breast cancer treatment, resistance develops in up to 50% of patients with advanced breast cancer. To combat resistance, targeted therapies have been approved for HR+ breast cancer. ER+ tumors are fueled by the hormone estrogen, and they can be treated with endocrine drugs that inhibit that process. Over the years, an array of related medications has arisen, including aromatase inhibitors, ER degraders (such as Faslodex), ER modifiers, and gonadotropin-releasing hormone agonists. Notably, drugs known as CDK4/6 inhibitors have hit the scene in the past decade, including palbociclib, ribociclib, and abemaciclib; in combination with aromatase inhibitors, these can prolong survival and prevent recurrence far more effectively than aromatase inhibitors alone. Still, many ER+ tumors eventually develop resistance to those combinations. Fortunately, they can now be treated with, yet another class of drugs known as PI3K inhibitors, and additional drugs are continuously introduced in clinical trials.
In the 2018-2032 forecast period, we expect a greater uptake of the CDK4/6 inhibitors [Ibrance/Palbociclib (Pfizer); Verzenio /abemaciclib (Eli Lilly) and Kisqali/ribociclib (Novartis)], targeted therapies such as Piqray/ alpelisib (Novartis Pharmaceuticals), Lynparza/Olaparib (AstraZeneca) and also the launch of the new drugs i.e., Chemotherapies -Ixempra/Ixabepilone (Allarity Therapeutics), AKT Inhibitors-Capivasertib (AstraZeneca), Selective Estrogen/androgen Receptor Degraders/modulators (SERDs/SERMs/SARMs)-Elacestrant (Radius Health/Menarini Group/Eisai Co. Ltd.), Imlunestrant (Eli Lilly and Company), Enobosarm (Veru Healthcare), Amcenestrant (Sanofi), Camizestrant (AstraZeneca), Giredestrant (Genentech), Lasofoxifene (SermonixPharmaceuticals), ARV-471 (Arvinas Pharmaceutical), Antibody drug conjugates (ADC)-Sacituzumab Govitecan-hziy (Gilead Sciences) and Datopotamab deruxtecan (AstraZeneca).
Report Highlights:
- ER+/HER2-mBC - Current Market Trends
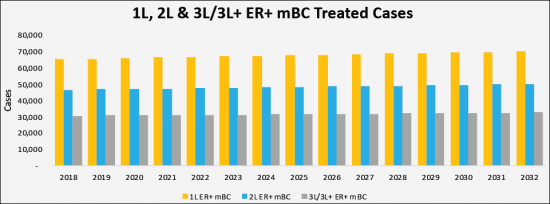
- ER+/HER2-mBC - Current & Forecasted Cases across the G7 Countries
- ER+/HER2-mBC- Market Opportunities And Sales Potential for Agents
- ER+/HER2-mBC - Patient-based Market Forecast to 2032
- ER+/HER2-mBC - Untapped Business Opportunities
- ER+/HER2-mBC - Product Positioning Vis-a-vis Competitors' Products
- ER+/HER2-mBC - KOLs Insight
Table of Contents
Executive Summary
- Key Findings
ER+/HER2- Metastatic Breast Cancer (mBC) Disease Background
- ER+/HER2- Metastatic Breast Cancer Definition
- Symptoms and Causes
- Pathogenesis
- Stages
ER+/HER2- Metastatic Breast Cancer (mBC) Diagnosis
- Diagnosis & Diagnostic Guidelines
- Biomarkers
- ESR1 Hotspot Mutations Lead to Resistance
Epidemiology and Patient Populations
- Key Findings
- Methods and data Sources
- Country Specific Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC) (US, Germany, France, Italy, Spain, UK, and Japan)
- Country Specific Incident Population with ER+/HER2- Metastatic Breast Cancer (mBC)
- Country Specific Treated Cases of ER+/HER2- Metastatic Breast Cancer (mBC) by Line of Therapies
Key Sources for ER+/HER2- Metastatic Breast Cancer (mBC) Epidemiology and Model Parameters
- United States
- United States Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- United States Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- United States Treated Cases of ER+/HER2- Metastatic Breast Cancer (mBC) by Line of Therapies
- Germany
- Germany Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- Germany Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- Germany Treated Cases of ER+/HER2- Metastatic Breast Cancer (mBC) by Line of Therapies
- France
- France Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- France Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- France Treated Cases of ER+/HER2- Metastatic Breast Cancer (mBC) by Line of Therapies
- Italy
- Italy Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- Italy Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- Italy Treated Cases of ER+/HER2- Metastatic Breast Cancer (mBC) by Line of Therapies
- Spain
- Spain Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- Spain Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- Spain Treated Cases of ER+/HER2- Metastatic Breast Cancer (mBC) by Line of Therapies
- United Kingdom
- United Kingdom Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- United Kingdom Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- United Kingdom Treated Cases of ER+/HER2- Metastatic Breast Cancer (mBC) by Line of Therapies
- Japan
- Japan Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- Japan Incident Populations with ER+/HER2- Metastatic Breast Cancer (mBC)
- Japan Treated Cases of ER+/HER2- Metastatic Breast Cancer (mBC) by Line of Therapies
Current Therapies and Medical Practice
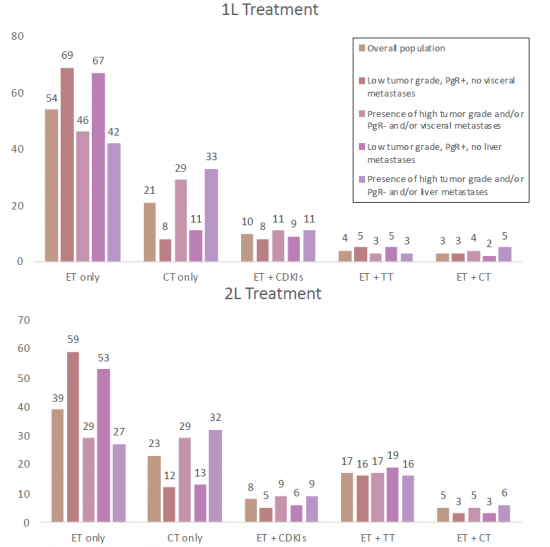
- Treatment & Medical Practices
- Benchmark Efficacy Data for CDK4/6 Inhibitors in 1L-3L ER+/HER2- mBC
- US Treatment Algorithm of Metastatic ER+ve Breast Cancer
- ER+/HER2- Metastatic Breast Cancer (mBC)-NCCN Treatment
- ER+/HER2+ Metastatic Breast Cancer (mBC)- NCCN Treatment Guidelines
- Treatment Algorithm of ER-positive/HER2-negative MBC- ESMO Guideline
- ER+/HER2- Metastatic Breast Cancer (mBC)- ESMO Guidelines
- KOLs Opinion on Current Treatment Option
ER+/HER2- Metastatic Breast Cancer (mBC)- Treatment Studies
- Endocrine therapy as a first-line treatment for ER+/HER2- Metastatic Breast Cancer in United States
- Real-world treatment patterns in a subset of HR+/HER2- advanced breast cancer patients with poor prognostic factors
- Preferred treatment sequences for HR+/HER2- Advanced Breast Cancer in Spain, France, Italy and Germany
- First-line treatment patterns in HR+/HER2- locally advanced or metastatic breast cancer in France, Germany, Italy, and Spain
Unmet Needs
ER+/HER2- Metastatic Breast Cancer (mBC)- Marketed Drug Chapters
- Benchmarking Studies
- Marketed Drug Chapters
- Ibrance/Palbociclib (Pfizer)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Verzenio /abemaciclib (Eli Lilly)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Kisqali/ribociclib (Novartis)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Ibrance/Palbociclib (Pfizer)
Emerging Therapies
- Pipeline Overview
- Therapeutic Developments Pipeline for ER+/HER2- Metastatic Breast Cancer (mBC)
- Product Analysis
- Camizestrant (AstraZeneca)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Giredestrant (Genentech)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Elacestrant (Radius Health/Menarini Group/Eisai Co. Ltd.)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Enobosarm (Veru Healthcare)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Imlunestrant (Eli Lilly and Company)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Amcenestrant (Sanofi)
- Product Profile
- Clinical Development
- Sales & Market Opportunity by 2032
- Capivasertib (AstraZeneca)
- Product Profile
- Clinical Development
- Datopotamab deruxtecan (AstraZeneca)
- Product Profile
- Clinical Development
- Lerociclib (G1 Therapeutics/EQRx/Genor Biopharma)
- Product Profile
- Clinical Development
- Sacituzumab govitecan (Gilead Sciences)
- Product Profile
- Clinical Development
- Lasofoxifene (Sermonix Pharmaceuticals)
- Product Profile
- Clinical Development
- ARV-471 (Arvinas Pharmaceutical)
- Product Profile
- Clinical Development
- Camizestrant (AstraZeneca)
- Product Analysis
ER+/HER2- Metastatic Breast Cancer (mBC)- Pricing & Reimbursement
Future Treatment Paradigm
- ER+/HER2- Metastatic Breast Cancer (mBC) Competitor Landscape and Approvals Anticipated
- Future Treatment Algorithms and Competitor Positioning
- Key Data Summary for Emerging Treatment
Annual Cost of Current & Emerging Therapies
Market Outlook
- Key Findings
Country Specific Market Forecast to 2032
- Sales of Drugs to Treat ER+/HER2- Metastatic Breast Cancer (mBC) in the Major Pharmaceutical Markets, 2018-2032
- Patient Share of ER+/HER2- Metastatic Breast Cancer (mBC) Therapies and by Drug
Market Forecast by Country
- United States
- United States Market for ER+/HER2- Metastatic Breast Cancer (mBC) 2018-2032 (USD Million)
- United States Market for ER+/HER2- Metastatic Breast Cancer (mBC) by Therapies 2018-2032 (USD Million)
- Germany
- Germany Market for ER+/HER2- Metastatic Breast Cancer (mBC) 2018-2032 (USD Million)
- Germany Market for ER+/HER2- Metastatic Breast Cancer (mBC) by Therapies 2018-2032 (USD Million)
- France
- France Market for ER+/HER2- Metastatic Breast Cancer (mBC) 2018-2032 (USD Million)
- France Market for ER+/HER2- Metastatic Breast Cancer (mBC) by Therapies 2018-2032 (USD Million)
- Italy
- Italy Market for ER+/HER2- Metastatic Breast Cancer (mBC) 2018-2032 (USD Million)
- Italy Market for ER+/HER2- Metastatic Breast Cancer (mBC) by Therapies 2018-2032 (USD Million)
- Spain
- Spain Market for ER+/HER2- Metastatic Breast Cancer (mBC) 2018-2032 (USD Million)
- Spain Market for ER+/HER2- Metastatic Breast Cancer (mBC) by Therapies 2020-2030 (USD Million)
- United Kingdom
- United Kingdom Market for ER+/HER2- Metastatic Breast Cancer (mBC) 2018-2032 (USD Million)
- United Kingdom Market for ER+/HER2- Metastatic Breast Cancer (mBC) by Therapies 2018-2032 (USD Million)
- Japan
- Japan Market for ER+/HER2- Metastatic Breast Cancer (mBC) 2018-2032 (USD Million)
- Japan Market for ER+/HER2- Metastatic Breast Cancer (mBC) by Therapies 2018-2032 (USD Million)
Market Drivers and Constraints
- What Factors Are Driving the Market for ER+/HER2- Metastatic Breast Cancer (mBC)?
- What Factors Are Constraining the Market for ER+/HER2- Metastatic Breast Cancer (mBC)?
 2030年全球乳癌藥物市場預測:依癌症類型、通路、最終用戶和地區進行分析
2030年全球乳癌藥物市場預測:依癌症類型、通路、最終用戶和地區進行分析 乳癌治療藥物市場:治療方法、癌症階段和銷售管道- 全球預測 2024-2030
乳癌治療藥物市場:治療方法、癌症階段和銷售管道- 全球預測 2024-2030 粗針穿刺切片市場規模、佔有率、趨勢分析報告:按技術、最終用途、地區、細分市場預測,2023-2030 年
粗針穿刺切片市場規模、佔有率、趨勢分析報告:按技術、最終用途、地區、細分市場預測,2023-2030 年 全球乳癌市場:按類型、治療類型、最終用戶和地區劃分的評估、機會和預測(2016-2030)
全球乳癌市場:按類型、治療類型、最終用戶和地區劃分的評估、機會和預測(2016-2030) 乳癌治療市場 - 依治療方式(標靶治療、荷爾蒙治療、化療、免疫治療),全球預測,2023-2032 年
乳癌治療市場 - 依治療方式(標靶治療、荷爾蒙治療、化療、免疫治療),全球預測,2023-2032 年 全球乳癌市場規模、佔有率和成長分析:按癌症和配銷通路- 行業預測(2023-2030)
全球乳癌市場規模、佔有率和成長分析:按癌症和配銷通路- 行業預測(2023-2030) 乳癌治療市場規模和預測、全球和區域佔有率、趨勢和成長機會分析報告範圍:按藥物治療、乳癌類型、配銷通路和地理位置
乳癌治療市場規模和預測、全球和區域佔有率、趨勢和成長機會分析報告範圍:按藥物治療、乳癌類型、配銷通路和地理位置 全球乳癌治療藥物市場-產業趨勢與預測(截至2030年)
全球乳癌治療藥物市場-產業趨勢與預測(截至2030年) HER2 低轉移性乳癌市場:Tumor Deck
HER2 低轉移性乳癌市場:Tumor Deck HER2 低表達乳癌 - 研發管線分析:2023 年
HER2 低表達乳癌 - 研發管線分析:2023 年